Silicone Oil Deposits on an Accommodating IOL
CASE PRESENTATION
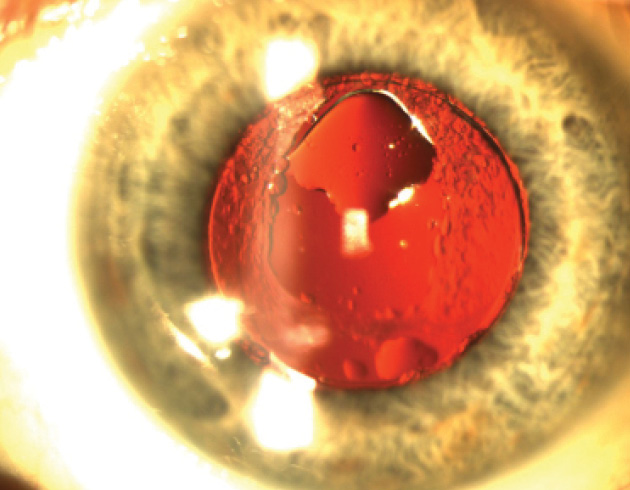
Figure 1. Silicone oil adheres superiorly to the posterior surface of a well-positioned Crystalens in an eye with an open posterior capsule.
A 54-year-old man presents with a complaint of blurred vision in his left eye. The patient underwent bilateral cataract surgery and implantation of a Crystalens (Bausch + Lomb) in 2012. He subsequently experienced a macula-off retinal detachment (RD) in his left eye and underwent repair with silicone oil in February 2014. The silicone oil was removed 7 or 8 months ago. He presents for a second opinion regarding silicone oil deposits on the Crystalens in his left eye.
The patient states that, since the repair of his RD, he has had “wavy” vision. He says that he can read the letters during an examination but finds that he sees a “ridge line” of contrast when looking into the distance, especially when there is a light background. He adds that, unlike with his right eye, images appear to swim sometimes, and he complains of some floaters since the silicone oil was removed. He would like to know if anything can be done or if this is “as good as his vision will be.”
Upon examination, the patient’s distance UCVA measures 20/25 OU, his intermediate UCVA is J1+ OU, and his near UCVA is J3 OU. Manifest refractions are -0.25 +0.25 × 022 = 20/20 OD and -0.25 = 20/25 OS. A slit-lamp examination shows a clear cornea, quiet anterior chamber, and well-positioned IOL in his left eye with an open capsule and silicone oil adherent to the posterior surface of the lens (Figure 1).
How would you proceed? Would you recommend an IOL exchange, and if so, what would your approach be? Would you recommend consideration of a vitrectomy or another procedure to attempt to clear the silicone oil from this well-positioned IOL that also yields a good quantity of vision?
—Case prepared by Audrey R. Talley Rostov, MD.
UDAY DEVGAN, MD
I am amazed that this patient, despite having a macula-off RD that necessitated the use of silicone oil, has recovered such great vision. Although a silicone oil droplet can induce aberrations, part of his visual disturbance may also be due to the macular status, which is not expected to be completely normal after a detachment. The haptics of the Crystalens tend to adhere strongly to capsular tissue, which makes an IOL exchange problematic. In addition, the patient actually has good vision with this IOL despite the oil droplets.
His options are to live with his current situation or to undergo attempted removal of the adherent silicone oil droplets. As reported in the European literature, perfluorohexyloctane could be used as a solvent to remove this silicone oil droplet.1 A simpler approach would be to use hydroxypropyl methylcellulose 2%, which is sold in the United States as OcuCoat (Bausch + Lomb), and to mechanically sweep the cannula across the IOL’s surface while injecting the hydroxypropyl methylcellulose. The ophthalmic viscosurgical device would slowly displace the silicone oil droplet. This technique might require multiple syringes of OcuCoat, which comes packaged in a 1-mL size. Once the silicone oil had been removed from the optic and displaced from the eye, a traditional I/A handpiece could be used to flush out the hydroxypropyl methylcellulose. It should be noted that more silicone oil that was trapped in the eye might present and require the same treatment.
A. JAMES KHODABAKHSH, MD
This patient has excellent distance, intermediate, and reading vision but has significant dysphotopsia and glare dysfunction, because silicone oil droplets cling to the posterior surface of the Crystalens. It is a well-known fact that silicone oil and silicone lenses do not mix well.
The first step is to educate the patient on his situation. His cataract surgery was excellent, and the retinal surgeons did a great job of correcting his sight-threatening complication. The patient still has a visual acuity of 20/25, although he is experiencing “ridge line” dysphotopsia when looking into the distance.
If the patient can tolerate his vision, one option is to leave things alone. Depending on his personality and needs, this may be the best course. The eye has already undergone multiple surgeries, and the patient is at risk of further RD with any intraocular procedure.
A second option is a vitrectomy with an air/fluid exchange to remove any additional presenting oil and to aspirate the silicone oil from the posterior side of the lens. In my experience, however, this approach will not work and is probably not worth trying. There always seems to be more silicone oil, no matter how many times a surgeon attempts to remove it. This oil will migrate forward again and attach itself to the silicone lens.
My preference in this case would be to correct the patient’s problem at its root: the silicone lens. With the help of a vitreoretinal colleague, I would perform a combined case of vitrectomy and an IOL exchange. I would implant an acrylic three-piece IOL in the sulcus and capture the optic, if possible. In the figure, capsular support appears to be excellent, so I would not expect an iris suture or scleral anchor to be necessary. Prior to surgery, I would explain to the patient that he will lose his intermediate and near vision after the lens exchange.
TAL RAVIV, MD
The adherence of silicone oil to silicone IOLs is well described in the literature. Due to the strong adhesion, IOL exchange has been advocated in the past.
Given this patient’s excellent refractive outcome with the Crystalens, I believe that an attempt to remove the silicone oil droplets is warranted. Although I have no personal experience with such procedures, a few case reports and videos appear to illustrate effective techniques for removing these drops. One involves using a 25-gauge vitrectomy cutter to aspirate the drops,2 another uses a forceful jet of balanced salt solution from a cannula to pick the drops off into the vitreous for aspiration (Figure 2),3 and a third uses a lens hook to physically knock off the drops.4 I hope that a local retina specialist takes on this case and uses these or another method.
Should such attempts fail, a discussion of the risks and benefits of an IOL exchange could be held with the patient and a monofocal acrylic IOL placed.
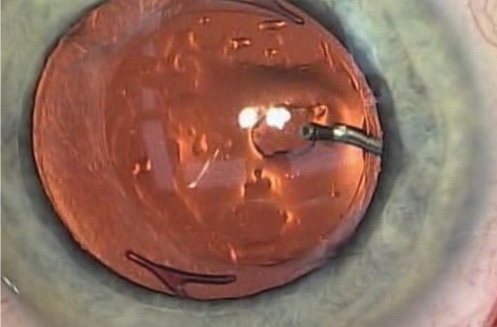
Figure 2. A “hydraulic squeegee” is created by bending a 30-gauge cannula at a 90º angle, very close to its tip. The modified instrument directs a forceful jet of BSS directly at the posterior side of the IOL to dislodge adherent silicone oil.
JEFFREY WHITMAN, MD
I would find out what the patient’s goal is. Even with his good postoperative visual acuity, perfect vision is not a realistic target based on his history of a macula-off RD, which may be the cause of the visual distortion. If, knowing this, the patient still wished to proceed with further intervention, I would advise him that I would try to clear the silicone oil from the lens but that, if doing so proved impossible, I would perform an IOL exchange.
Upon entering the eye, I would place viscoelastic anterior and posterior to the lens and then attempt to “power wash” the lens with BSS (Alcon) on a cannula. I have found that this method can displace the silicone oil (it floats into the anterior chamber, where it can be aspirated) and avoid further surgery. If the oil remained, I would use microscissors and a micrograsper (both from MicroSurgical Technology) to cut the lens distal to the hinge on either side (again, away from the optic). I would leave the stumps and remove the central body. A three-piece acrylic lens could then be placed in the sulcus.
1. Langefeld Í, Kirchhof B, Meinert H, et al. A new way of removing silicone oil from the surface of silicone intraocular lenses. Graefes Arch Clin Exp Ophthalmol. 1999;237(3):201-206.
2. Sakimoto S, Tsukamoto Y, Saito Y. Removal of silicone oil droplet adhering to a silicone intraocular lens using 25-gauge instrumentation. J Cataract Refract Surg. 2009;35:383-385.
3. Riemann C. Removal of silicone oil from an IOL using the “hydraulic squeegee.” Eyetube.net. http://eyetube.net/v.asp?f=hosolo. Posted September 8, 2009. Accessed July 30, 2015.
4. Kageyama T, Yaguchi S. Removing silicone oil droplets from the posterior surface of silicone intraocular lenses. J Cataract Refract Surg. 2000;26:957-959.
Section Editor Lisa Brothers Arbisser, MD
• emeritus position at Eye Surgeons Associates, the Iowa and Illinois Quad Cities
• adjunct associate professor, John A. Moran Eye Center, University of Utah, Salt Lake City
Section Editor Audrey R. Talley Rostov, MD
• private practice with Northwest Eye Surgeons, Seattle
• medical advisory board, SightLife, Seattle
• (206) 528-6000; atalleyrostov@nweyes.com
Uday Devgan, MD
• private practice, Devgan Eye Surgery, Los Angeles
• clinical professor of ophthalmology, Jules Stein Eye Institute, UCLA
• chief of ophthalmology, Olive View UCLA Medical Center
• (800) 377-1969; devgan@gmail.com; Twitter @devgan
• financial disclosure: consultant to and speaker for Bausch + Lomb A. James Khodabakhsh, MD
• clinical assistant professor of ophthalmology, New York Medical
College, Valhalla, New York
• surgical director, Beverly Hills Vision Institute, Beverly Hills, California
• managing partner, Specialty Surgical Center, Beverly Hills, California
• (310) 273-2333; lasereyedoc@aol.com
• financial disclosure: consultant to and speaker for Abbott Medical Optics and Bausch + Lomb
Tal Raviv, MD
• founder and medical director, Eye Center of New York
• clinical associate professor of ophthalmology, New York Eye and Ear Infirmary of Mount Sinai
• (212) 889-3550; talraviv@eyecenterofny.com; Twitter @TalRavivMD
• financial interest: none acknowledged
Jeffrey Whitman, MD
• president and chief surgeon, Key-Whitman Eye Center, Dallas
• (214) 754-0000
• financial disclosure: consultant to Alcon, Bausch + Lomb, and Oasis Medical Optics